
Resolution of a Juvenile Idiopathic Scoliosis (JIS) using a Low-Profile ScoliBrace and Scoliosis Specific Rehabilitation
Summary:
This case demonstrates the resolution of a moderate-sized Juvenile idiopathic scoliosis in an 11-year- old male patient using a ScoliBrace orthosis combined with scoliosis specific rehabilitation. The patient was skeletally immature at the time of presentation and had a clinically relevant leg length discrepancy that was contributing to his deformity. The patient had a 30° left lumbar and a 15 degree right thoracic curve. The patient was prescribed a low-profile ScoliBrace orthosis, scoliosis specific rehabilitation, and a heel/shoe lift to normalize the length of the limbs. The patient was compliant with the wearing of the brace and the heel lift, but less conscientious with his exercise prescription.
After 11 months of treatment, the patient’s curves had been reduced to <10°. The patient is out of the brace and continuing to use the heel lift in conjunction with exercise rehabilitation. It is hoped that continued conservative management will help to stabilize the excellent result that has been for this patient.
Case Background
The patient presented to the ScoliCare clinic at age 11 years for assessment of an idiopathic scoliosis that had been diagnosed by a paediatrician 5 years earlier. The patient had been referred by their local chiropractor. Both the patient and his mother had concerns that the scoliosis would progress. The young man had been experiencing 4/10 lower back pain (LBP) on occasion that was exacerbated by prolonged standing.
The patient had been receiving chiropractor care for the management of the LBP, but no treatment to specifically address the scoliosis. The patient was involved with Judo and Brazilian Ju Jitsu for approximately eight hours per week.
Examination Findings
The patient was a healthy young male and the systems review was unremarkable. The medical history was normal except for a buckle fracture of the wrist and a positive family history of scoliosis. Domain scores on the Scoliosis Research Society questionnaire (SRS-22r) were reduced compared to normative data across all domains (Function = 3.4, Pain = 3.8, Self-image = 4.0 Mental health = 3.2).
The physical examination revealed an obvious left lumbar curvature of the spine and a compensatory right thoracic curve. There was a positive Adam’s Forward bend test with an angle of trunk rotation measuring 5° and 10° in the mid-thoracic and lumbar spine respectively. Clinical tests for leg-length inequality (LLI) indicated a short left-leg (approximately 20mm) relative to the right leg (Figure 1).
Scoliometer measurements over the pelvis with the patient in the flexed position produced a reading of 8°. X-rays taken soon after the initial consultation at the ScoliCare clinic highlighted a primary left lumbar scoliosis measuring 30° Cobb, a compensatory left thoracic curve with a magnitude of 15° Cobb and un-leveling of the pelvis and sacral base (Figure 2). X-ray evaluation of the LLI indicated that a 28mm lift would be required to level the pelvis.

Figure 1: Posteroanterior postural photograph (Left), Posteroanterior postural photograph with a 28mm leg lift (Middle), Relative leg length inequality [Weber-Barstow test] (Right).

Figure 2: Posteroanterior x-ray (Stitched) indicating a 30° left lumbar scoliosis and pelvic/sacral un-levelling and a 15° right thoracic scoliosis. Note: the patient is not wearing a shoe or heel lift in the plain films above.
Intervention
The patient was prescribed a ScoliBrace low-profile, rigid, thoraco-lumbo-sacral orthosis [TLSO] (Figure 3), and scoliosis specific rehabilitation. Part-time brace wear (16 hours per day) was advised and the patient was instructed to use the ScoliRoll traction-fulcrum device (Figure 3) on the primary and secondary curves.
The other component of the rehabilitation program involved Scientific Exercise Approach to Scoliosis (SEAS) rehabilitation exercises performed daily. In addition to the brace and the rehabilitation procedures, the patient was also recommended to wear a shoe lift (20mm) and a heel lift (8mm) to address the leg length discrepancy. The patient was also provided with an ischial lift to use whenever seated to counter the effects of the sacral/pelvic obliquity on the patient’s curves.

Figure 3: Posteroanterior photograph of the patient wearing the TLSO including the shoe and heel lift (Left), Side-lying photograph of the patient using the ScoliRoll device on the apex of the lumbar scoliosis (Right).
Outcomes
The patient was compliant with the bracing and rehabilitation program, and consistently used the shoe and heel lift. Out-of-brace x-rays, with the patient wearing their shoe and heel lift, taken one month after the brace fitting highlighted a dramatic reduction in the primary and secondary curves (Figure 4 – Left).
Out-of-brace plain films, without shoe and heel lifts, taken seven months after starting the bracing showed a maintenance of the correction. However, the patient reported that he had been less conscientious with the performance of the SEAS exercises and the use of the ScoliRoll in the period leading up to this review. It is important to note that the patient was still Risser 0, 7 months after the initiation of treatment.
The patient was counselled regarding the importance of the exercises and use of the ScoliRoll.
Attempts were made to renew the patient’s enthusiasm for the rehabilitation program, by modifying the exercises and making them more relevant to his martial arts training, and also checking in more frequently with the patient.
Out-of-brace x-rays taken 11 months after starting the treatment program demonstrated a correction of the patient’s curves to <10° Cobb with the patient wearing his heel/shoe lift (Figure 4 – Right).
The patient is currently still under care, however the most recent physical examination revealed that the patient’s posture was looking considerably more balanced and the angle of trunk rotation measured at 4° in the thoracic spine and 0° in the lumbar spine with the patient wearing their heel lift.
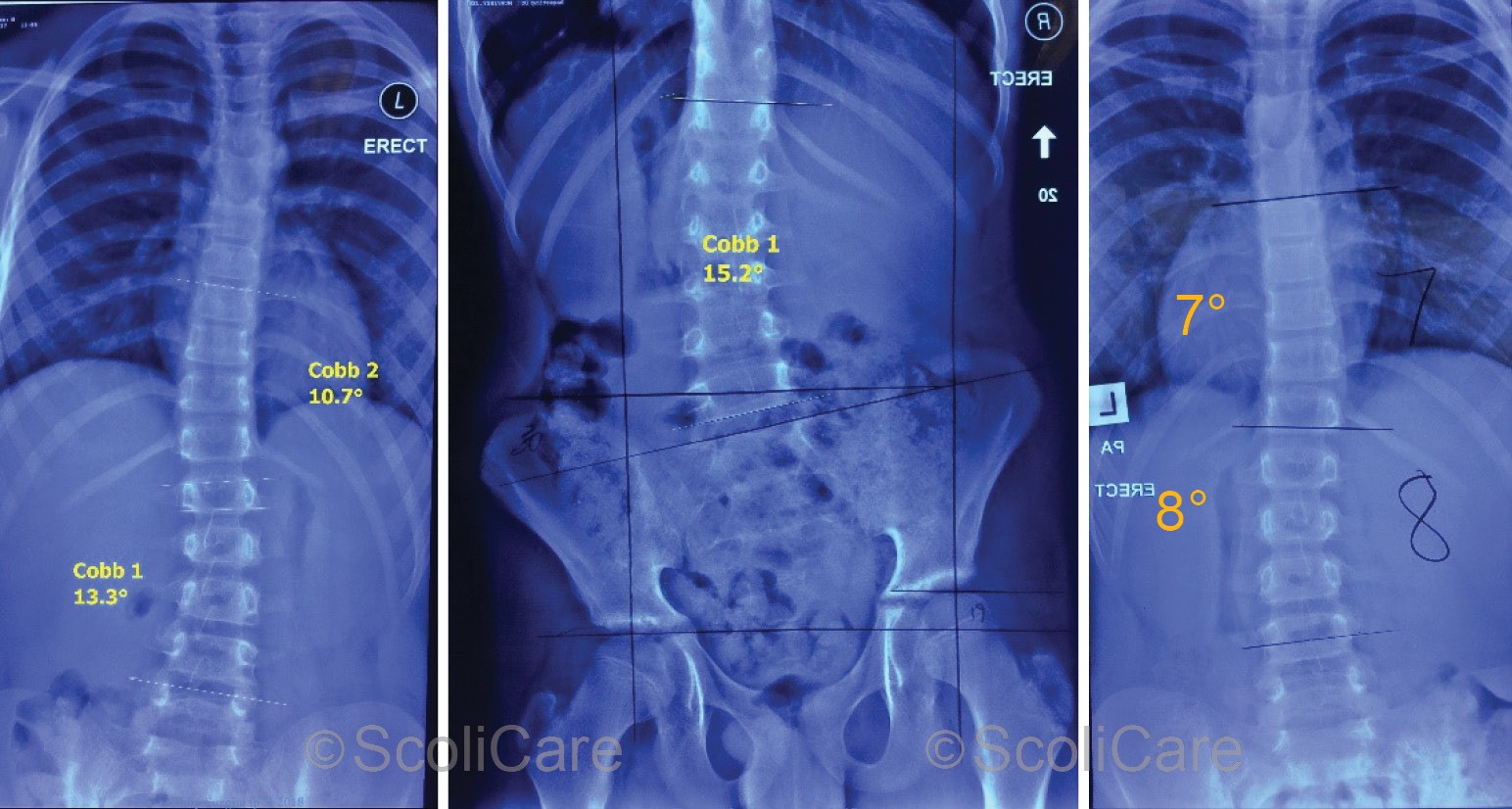
Figure 4: Posteroanterior 1-month out-of-brace x-ray with the patient wearing the shoe and heel lifts (Left), Posteroanterior 7-month out-of-brace x-ray without the shoe or heel lift (Middle), Posteroanterior 11-month out-of-brace x-ray with the shoe and heel lift (Right).
Discussion
This case is an example of an adolescent patient presenting with a progression of an untreated juvenile idiopathic scoliosis. The case is further complicated by the presence of a significant LLI. It is common for patients to have small differences in the length of their paired limbs.
Usually this difference in leg length from one side to another is less than 20mm and it is rare for differences of this magnitude to be clinically significant. However, LLI of >20mm places excessive stress on the hip, knee, sacroiliac joint and lumbar spine and significantly alter the normal gait kinematics.
Even small changes in the length of one leg compared to the other may cause pelvic obliquity which can lead to a functional scoliosis in the lumbar spine. The subject of this case study had a LLI of approximately 28mm which was likely contributing to pain and discomfort. The correction of the LLI with a shoe and heel lift corrected the functional component of the patient’s deformity but did not result in a correction of the observed structural deformity.
The ScoliBrace TLSO and scoliosis specific rehabilitation were used to correct the residual curvature in the lumbar and thoracic spine that remained after the pelvis had been leveled.
Conclusion
This case demonstrates the reduction of a juvenile idiopathic scoliosis presenting in an adolescent patient with a significant LLI using a ScoliBrace orthosis, scoliosis specific rehabilitation and shoe and heel lifts. The ScoliBrace TLSO and scoliosis specific rehabilitation were used to correct the residual curvature in the lumbar and thoracic spine that remained after the pelvis had been leveled.
NB: Results vary from case to case. Our commitment is to recommend the most appropriate treatment based on the patients type and severity of scoliosis.