
Reduction of a severe scoliosis using ScoliBrace in a Young Female Gymnast
Summary:
This case details the successful management of a young female gymnast with severe adolescent idiopathic scoliosis (AIS) using a ScoliBrace orthosis and physiotherapeutic scoliosis specific exercise. The patient initially presented to the ScoliCare clinic at age 14 with a 71° right thoracic curve and a 40° left lumbar curve. There were obvious distortions to the patient’s posture – specifically right coronal imbalance and associated waist curve asymmetry. The patient had been unresponsive to manual therapy intervention and had refused surgery.
The patient was prescribed a ScoliBrace rigid thoracolumbosacral orthosis (TLSO) combined with scoliosis specific exercise. After 18 months of bracing and scoliosis specific exercise the patient’s curves had been reduced from 71° down to 56° in the thoracic spine and from 40° down to 32° in the lumbar spine. The patient’s posture and coronal imbalance was also significantly improved at the end of the treatment program.
Case Background
The patient was a 14-year-old, high-level, competitive gymnast. The patient’s mother had noticed a curvature in her daughter’s spine and taken her to see a manual therapist. The therapist had made a diagnosis of Adolescent Idiopathic Scoliosis (AIS) and treated the patient for three months. Unfortunately, the patient had not responded to treatment and was referred to the ScoliCare Clinic for an assessment.
Examination Findings
The examination revealed some significant postural changes. Specifically, notable curvature in the middle and lower sections of the patient’s spine, uneven heights of the pelvic bones, and torsion of the rib cage (Figure 1).
X-rays taken at the time showed a large 71° curve in the thoracic spine and a secondary curve, measuring 40°, in the lumbar spine (Figure 1). The patient was only Risser 2, indicating that she still had a significant amount of growing to do.
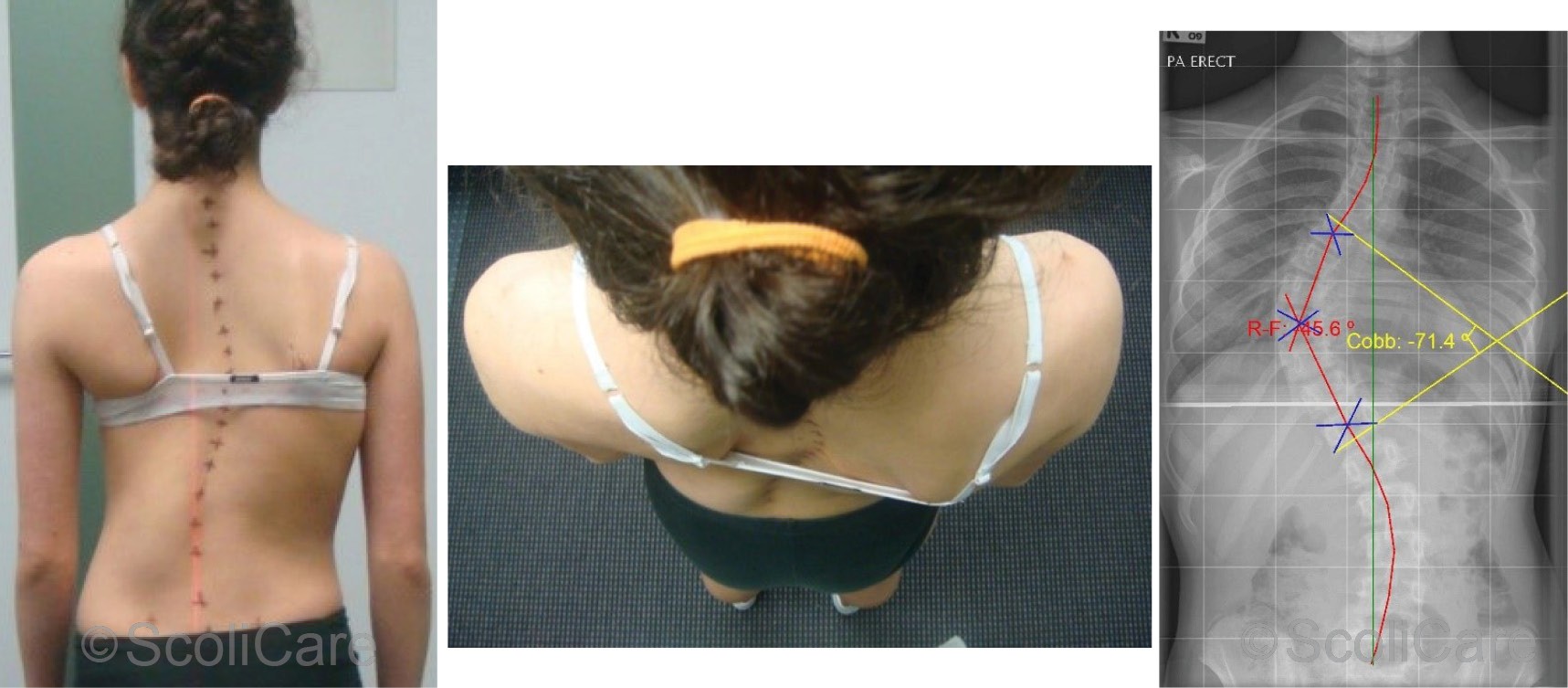
Figure 1: A) Posterior-anterior view highlighting the scoliosis and pelvic tilt.
B) Superior to inferior view highlighting torsion of the rib cage associated with the thoracic spine curvature.
C) Posterior-anterior x-ray demonstrating the curvature of the spine and changes in the rib cage.
Intervention
As both the curves were quite large, and the patient was skeletally immature, it was recommended that the patient be seen by an orthopaedic surgeon. The surgeon’s recommendation was that the patient undergo surgery to correct the abnormal spinal curvatures. After careful consideration, both the patient and her parents declined the surgeon’s recommendation. Instead, they decided to go with a more conservative approach.
The patient was subsequently prescribed a custom-made ScoliBrace (Figure 2), and rehabilitation exercises based on the Schroth principles. The recommendation was that the patient be braced for two years until she stopped growing. A daily scoliosis specific exercise program was designed for the patient to support the corrections being made by the brace. New exercises were added to the program as the patient progressed. Regular follow-ups were scheduled to ensure that A) the patient was responding to the treatment, and B) to monitor compliance with the bracing and exercise program.

Figure 2: Patient wearing the ScoliBrace
Outcomes
The patient’s spine responded favourably to the treatment with one-month x-rays showing that the larger curve could be reduced from 71° down to 40° with the patient wearing the brace (Figure 2).
In total, the patient was braced for 18 months. The patient also participated in supervised exercise sessions at the clinic and performed similar exercises at home. At the end of the treatment period, the patient’s curves had reduced significantly (71° to 56°) as demonstrated in the out-of-brace x-rays in Figure 3. The patient’s posture was also notably improved.
In total, the patient was braced for 18 months. The patient also participated in supervised exercise sessions at the clinic and performed similar exercises at home. At the end of the treatment period, the patient’s curves had reduced significantly (71° to 56°) as demonstrated in the out-of-brace x-rays in Figure 4. The patient’s posture was also notably improved.
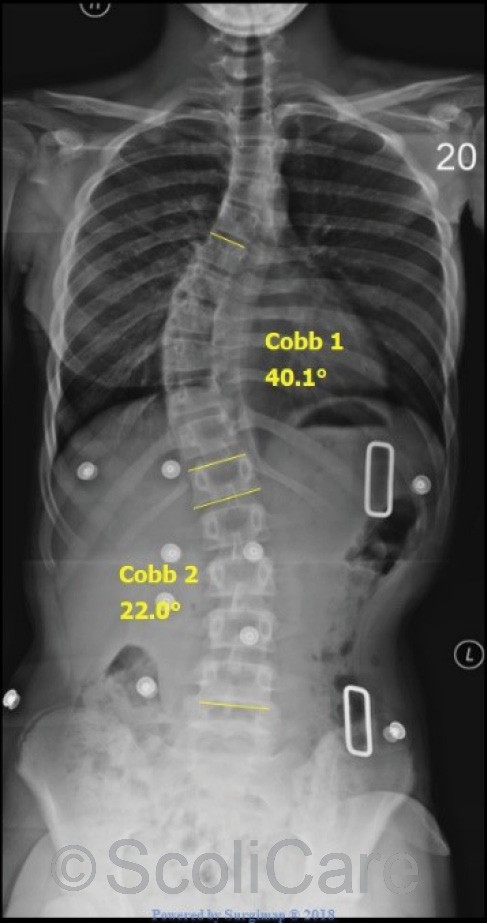
Figure 3: In-brace frontal x-rays taken one month after the brace fitting.
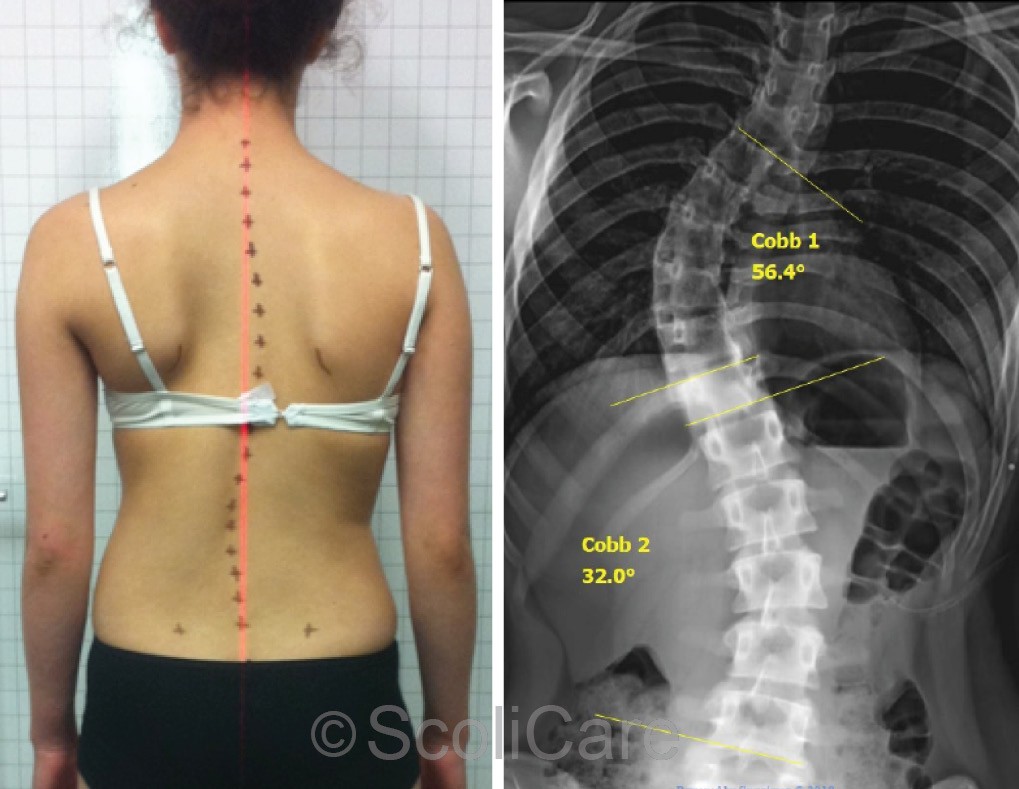
Figure 4: Out of brace x-ray
Discussion
Normally, brace treatment is reserved for AIS patients with moderate (20-45°) scoliotic curves. Scoliosis specific exercise rehabilitation is used in mild (10-20°) scoliosis as a standalone treatment, and as a supplement to bracing in patients with moderate scoliosis. Patients with more severe scoliosis are typically managed surgically. There is very little research to support the use of bracing or exercise in patients with curves exceeding 45°.
This case is unique in the sense that the patient/parents refused surgery and elected to try a more conservative option. Care was taken to explain to the patient/parents that surgical treatment is the recommended pathway for AIS patients with severe curves. The is a scarcity of evidence to support the use of bracing in curves >60° in this population.
Conclusion
This case demonstrates the reduction of a severe scoliosis in an AIS patient who declined surgical intervention.
NB: Results vary from case to case. Our commitment is to recommend the most appropriate treatment based on the patients type and severity of scoliosis.