
Correction of a moderate thoracolumbar scoliosis using a ScoliNight orthosis and Scoliosis Specific Rehabilitation
Summary:
This case demonstrates the successful treatment of a 12-year-old girl presenting with a mild scoliosis. The patient presented with a 19° thoracolumbar curve. The patient was prescribed a custom, rigid ScoliNight brace, and scoliosis specific rehabilitation which included exercise and use of the ScoliRoll spinal orthosis.
The patient wore the brace at night for nine months in conjunction with daily rehabilitation. At the end of the bracing period, the patient’s curve had reduced to 8° out-of-brace. At the time of the most recent follow-up appointment (26 months after starting treatment), the patient’s posture looks symmetrical with little evidence of scoliosis.
Case Background
The patient was referred to the ScoliCare clinic at age 12. The patient had been experiencing lower back pain on and off for several years, and the patient’s mother had noticed some deformity in her child’s spine. Consultation with the local chiropractor and the GP, when the patient was 8 years old, had confirmed the presence of a small thoracolumbar scoliosis (12° Cobb).
The patient had not received any treatment for her scoliosis, but instead was being observed at regular intervals by the GP/chiropractor. The patient was quite physically active with involvement in a variety of activities (dance, gym, cross country running, Oz tag, netball, and swimming).
Examination Findings
The patient reported a probable family history of scoliosis with both her mother and father experiencing back pain and showing signs of spinal deformity.
The patient completed the Scoliosis Research Society questionnaire (SRS-22r), which revealed decreased scores compared to normal in the pain and self-image domains.
Upon examination, there was a left curvature of the spine in the thoracolumbar region, apparent pelvic obliquity, and the appearance of an increase in the kyphosis angle in the thoracic spine (Figure 1).
The patient had a set of recent x-rays (Figure 2) that showed a left 19° thoracolumbar scoliosis with an apex at T12. The patient’s thoracic kyphosis measured 42° which is in the high normal range (20-45°) for her age.
These x-rays demonstrated a clinically significant progression in the patient’s scoliosis since the last radiographic review. The tri-radiate cartilage was still open on these films indicating that the patient was Risser 0 and still had a substantial amount of growth ahead of her.
A diagnosis of juvenile idiopathic scoliosis with progression in adolescence was made.

Figure 1: Lateral postural photographs (Left), Posteroanterior postural photograph (Right).
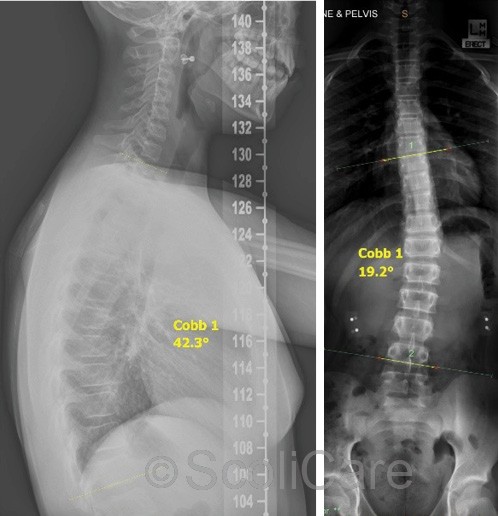
Figure 2: Lateral x-ray with a kyphosis angle measuring 42° (Left), Posteroanterior full spine x-ray demonstrating a 19° thoracolumbar scoliosis (Right)
Intervention
The patient was advised that scoliosis specific rehabilitation and a rigid brace would be the most suitable treatment for her spinal deformity. However, the patient was hesitant to wear a brace.
Taking into account the magnitude of the patient’s scoliosis and the patient’s reluctance to wear a standard brace, a night-time thoracolumbosacral orthosis [TLSO] (ScoliNight brace) was suggested (Figure 3).
The patient was required to wear the brace while sleeping and for 4 additional hours per night (Total 16 hours).
Scientific Exercise Approach to Scoliosis (SEAS) rehabilitation exercises and home fulcrum-traction using the ScoliRoll orthotic device were also recommended. The patient was instructed to perform the rehabilitation exercises and use the ScoliRoll each day.

Figure 3: Posteroanterior photograph showing the patient wearing the ScoliNight orthosis (Left), Side-lying photograph of the patient on the ScoliRoll orthosis with the peak of the device positioned at the apex of the convexity of the patient’s thoracolumbar curve (Right).
Outcomes
The patient was compliant with the brace wear and reported that she had no difficulties sleeping in the orthosis.
Supine x-rays taken one month after the brace fitting revealed that the patient’s curve was over-corrected, to the point of being reversed to a right convex thoracolumbar curve measuring 16°, in the brace (Figure 4).
Postural analysis performed at this time illustrated that the patient’s posture was substantially improved. The dosage of bracing was reduced to nighttime (sleeping) only.
Standing out-of-brace x-rays taken 9 months after the brace fitting showed that the patient’s curve had been reduced to 8° and the patient was Risser 1 (Figure 4). The patient was weaned from the brace from this point and advised to continue with the scoliosis specific rehabilitation.
The patient is continuing to perform the SEAS exercises and use the ScoliRoll to stabilize the correction that has been obtained and maintain strength in the trunk muscles.
The patient’s posture is looking substantially more balanced with no evidence of trunk rotation (Figure 5).
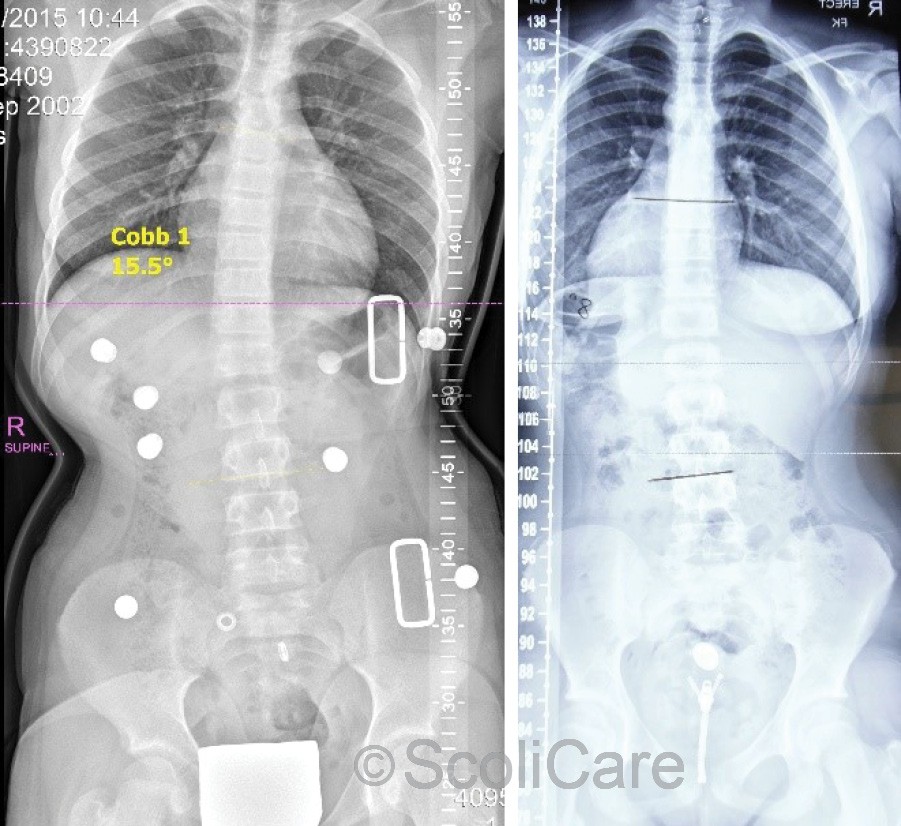
Figure 4: Supine anteroposterior x-ray highlighting that the patient’s scoliosis was over-corrected to 16° in-brace after 1 month (Left), Standing posteroanterior x-ray highlighting that the patient’s scoliosis was reduced to 8° out-of-brace after 9 months of brace wear (Right).

Figure 5: Lateral postural photograph (Left), Posteroanterior photograph (Middle), Adam’s forward bend test (Right).
Discussion
Night-time bracing offers a solution to patients with smaller curves, who have difficulty with full-time bracing regimens or find brace wear psychologically burdensome. The subject of this case expressed reluctance to wear a brace. If a standard TLSO at a full-time schedule was prescribed in this case there may have been issues with compliance. A less burdensome, part-time, the solution, however, posed no problem for the patient.
Night-time bracing is thought to work via many of the same principles as the standard TLSO treatments but is over-corrective in nature and is designed to be worn in a recumbent position.
This style of brace is able to achieve significant in-brace corrections (as demonstrated by the significant over-correction observed in this case) and is most effective for small to moderate curves (10-25°).
Patient’s typically required longer treatment time with night-time bracing, so it is advised that night-time bracing be implemented when the patient is in their early teens and still skeletally immature (Risser 0-2).
The combining of scoliosis-specific rehabilitation with night-time bracing is not well studied, but the practice is common in full-time bracing programs and it therefore likely to confer similar benefits.
Conclusion
This case study demonstrates the successful management of a moderate infantile idiopathic scoliosis using a ScoliBrace orthosis.
NB: Results vary from case to case. Our commitment is to recommend the most appropriate treatment based on the patients type and severity of scoliosis.