
Correction of a 61° Hyper-kyphosis using a KyphoBrace Orthosis
Author: Dr Jeb McAviney
Summary:
This case study details the correction of a hyper-kyphosis in a skeletally mature 16-year-old male. The patient’s primary reason for seeking treatment was pain, however, he was also bothered by the abnormal aesthetics associated with his spinal deformity.
At the time of the initial consultation, the patient had a thoracic kyphosis angle measuring 61°, a small thoracolumbar scoliosis, and a small leg-length inequality. The patient was diagnosed with Scheuermann’s kyphosis and prescribed a rigid KyphoBrace orthosis and a 10 mm heel lift for the scoliosis and the leg length discrepancy.
The patient wore the orthosis for 25 months for 20 hours each day and was compliant with the use of the heel lift. Follow-up x-rays performed six months after the cessation of brace-wear revealed that the thoracic kyphosis angle had been reduced to 43°, which is within normal range based on the patient’s sex and age.
Case Background
A 16-year-old male patient was referred to the ScoliCare clinic by a local Chiropractor. The patient had been experiencing pain in the mid-back and poor posture for the past year. The patient had gone through a rapid growth spurt in the two years prior to the consultation at the Scolicare clinic. The patient reported that he regularly played tennis, football, and computer games.
Examination Findings
The patient rated his mid-back pain, on average, as 2/10 on a visual analogue scale but stated that the pain was aggravated by sitting in car seats for long periods of time and could be as high as 5/10 at times.
The patient’s main concern was the noticeable curvature in his back. The patient was otherwise healthy.
The physical examination revealed a significant increase in the patient’s normal thoracic kyphosis (Figure 1) with associated stiffness in this area. There was focal angulation observed in the thoracic spine during the Adam’s forward bending test.
There was a small left curvature in the thoracolumbar spine that was noted along with an apparent leg length discrepancy. There were no other significant clinical findings. A working diagnosis of Scheuermann’s kyphosis was made and plain films were requested. The patient was Risser 5. A 61° hyper-kyphosis was noted with an apex at the T7/8 intervertebral disc level with no significant changes in vertebral body height (Figure 1).

Figure 1: Lateral full spine x-ray (left), Lateral postural photograph (middle), Adam’s forward bend (right).
Intervention
A specialized brace for the treatment of hyper-kyphosis (called a KyphoBrace [Figure 2]), was prescribed to aid in the reduction and stabilization of the patient’s spinal deformity.
It was recommended that the orthosis be worn for a minimum of 20 hours per day for a 24-month period. The patient has also been prescribed a 10 mm heel lift for correction of the thoracolumbar scoliosis. (Note: The patient is not wearing a heel lift in Figure 2).
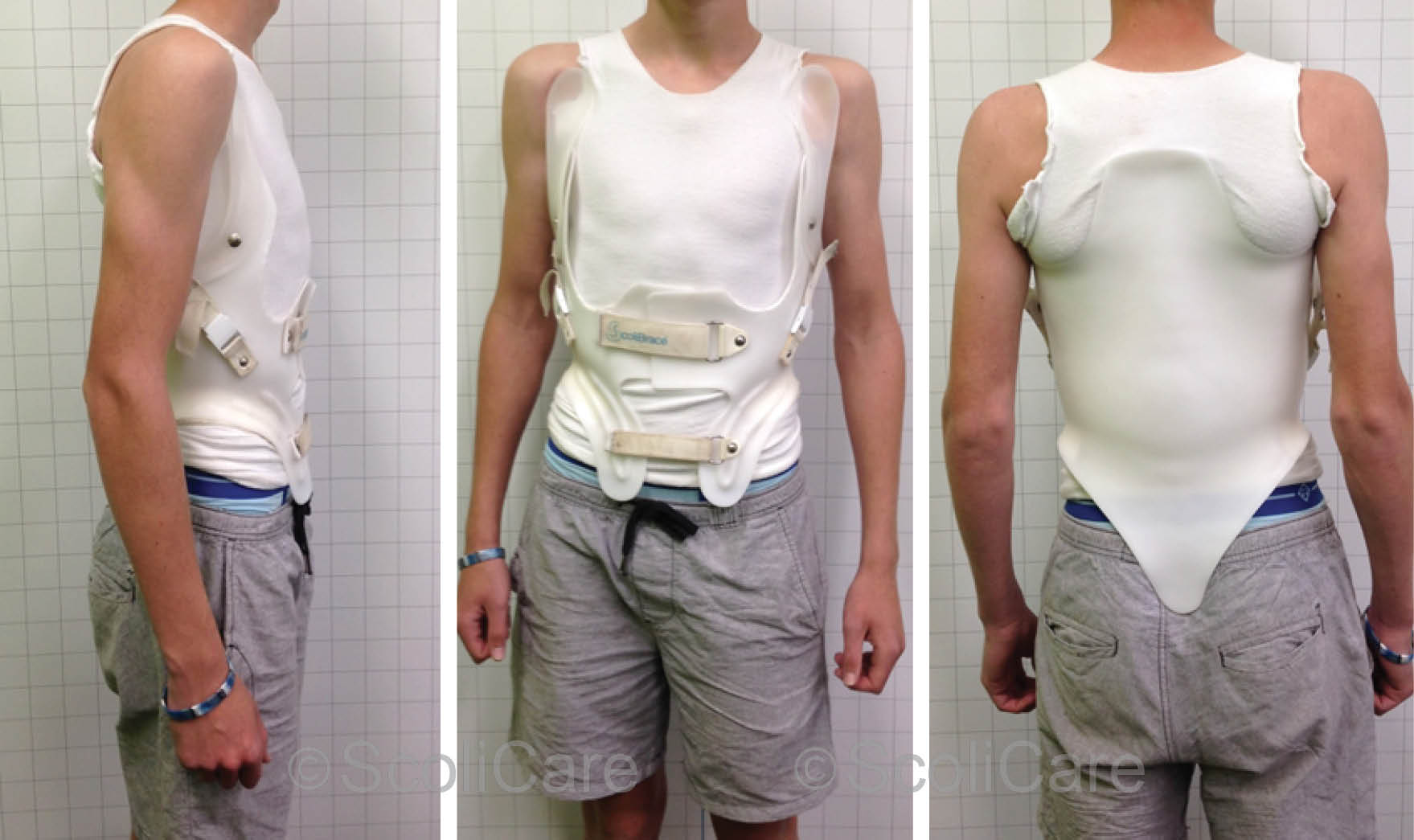
Figure 2: Lateral in-brace photograph (left) Anteroposterior in-brace photograph (middle), posteroanterior in-brace photograph (right).
Outcomes
The orthosis was well-tolerated by the patient, and he reported that he was compliant with the prescribed hours of bracing.
In-brace x-rays taken at the 3-month mark, demonstrated that the patient’s kyphosis had been reduced from 61° down to 47° (Figure 3 [Left]). Out-of-brace plain films taken 4 months into the treatment program highlighted that the curve was 48° (Figure 3 [Right]).
The patient continued to wear the brace for 25 months in total. Plain films taken 6 months after the cessation of brace wear revealed that the patient’s kyphosis had remained stable in the short-term at 43° (a reduction of 19° from the initial presentation) [Figure 4].
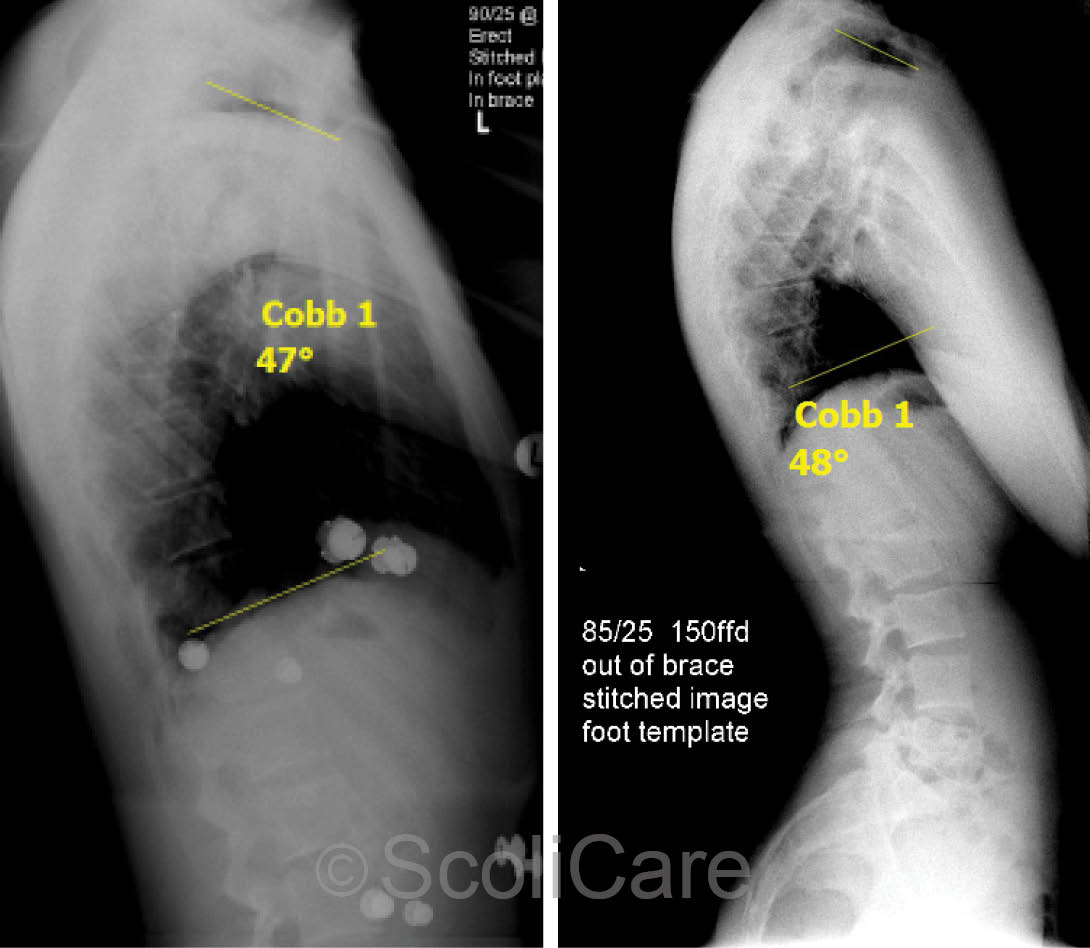
Figure 3: Three-month lateral in-brace x-ray highlighting a 47° kyphosis (Left), Four-month lateral out-of-brace x-rays demonstrating a 48° kyphosis (Right).
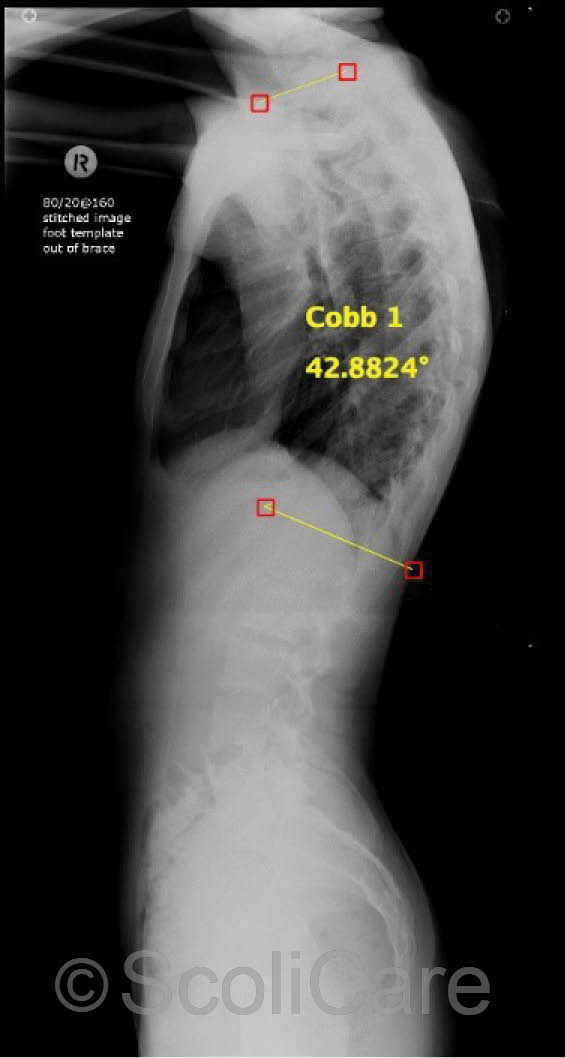
Figure 4: Plain film lateral x-rays taken 6 months after the cessation of brace wear. The kyphosis measured 43° at this time.
Discussion
The mean physiological curve in the thoracic spine measures 33° (±2 standard deviations = 20-50°)1 in adolescents and is influenced by age, gender, height, weight and genetic factors.
The thoracic kyphosis increases in size and stiffness as we age. This is in part due to changes in muscle tone, effects of occupational or habitual postures, changes in vertebral body shape, and bone mineral density.
It is, therefore, important to manage cases of hyperkyphosis in adolescent patients so as to minimize the effect of the natural deterioration that occurs with age. Furthermore, deleterious changes in the sagittal balance can result in pain, poor function, low self-image and decreased quality of life.
There is evidence to suggest that bracing is an effective treatment for patients with hyper-kyphosis. The best results from bracing are observed when treatment is initiated in skeletally immature patients who have curvatures of between 55-80°.
This case is unique in the sense that the patient had already transitioned through the period of peak growth velocity and was Risser 5 at the initiation of treatment. Despite this, a significant correction was still achieved, which resulted in the patient’s kyphosis being shifted from a pathological curvature to normal range kyphosis angle for the patient’s age.
Conclusion
This case demonstrates that the KyphoBrace may be used to stabilize/reduce hyper-kyphosis in adolescent patients.
References:
1. Boseker, E.H., et al., Determination of “normal” thoracic kyphosis: a roentgenographic study of 121 “normal” children. J Pediatr Orthop, 2000. 20(6): p. 796-8.
NB: Results vary from case to case. Our commitment is to recommend the most appropriate treatment based on the patients type and severity of scoliosis.